|
TRANSLATE THIS ARTICLE
Integral World: Exploring Theories of Everything
An independent forum for a critical discussion of the integral philosophy of Ken Wilber
  Frank Visser, graduated as a psychologist of culture and religion, founded IntegralWorld in 1997. He worked as production manager for various publishing houses and as service manager for various internet companies and lives in Amsterdam. Books: Ken Wilber: Thought as Passion (SUNY, 2003), and The Corona Conspiracy: Combatting Disinformation about the Coronavirus (Kindle, 2020). Frank Visser, graduated as a psychologist of culture and religion, founded IntegralWorld in 1997. He worked as production manager for various publishing houses and as service manager for various internet companies and lives in Amsterdam. Books: Ken Wilber: Thought as Passion (SUNY, 2003), and The Corona Conspiracy: Combatting Disinformation about the Coronavirus (Kindle, 2020). TABLE OF CONTENTS | REVIEWS
Where Are All These PCR ‘False Positives’ Anyways?The Corona Conspiracy, Part 29Frank Visser
Doubting the existence of the SARS-CoV-2 virus and/or the reliability of PCR tests has become thoroughly obselete.
If there is one rumor that keeps rearing its ugly head during this worldwide COVID-19 pandemic it is that the PCR tests testing for SARS-CoV-2 are unreliable because they primarily produce "false positives". A false positive in this context means: the test outcome may be positive, but you don't really have that virus. This undermines the trust in science, and in the government policies that base themselves on this very science. Is there any truth to this claim? Or is it a fallacy, a fairy tale, a lie that needs to die? On false positivesJust to give you an idea about what it is exactly that is denied by this spurious claim, let's present first the view of conventional science. We have a global pandemic at hand caused by a new virus, related to the SARS family of viruses. A PCR test has been developed that can detect a highly specific fragment of this virus, or at least of this particular family of viruses. These tests usually have a percentage of positive outcomes, the "positive rate", between 0 and 25%, though the WHO recommends 5% as an indication that the pandemic is under control.[1] Of course, this highly depends on the population you are testing: those with clear COVID-19 symptoms or randomly the population at large. The fact that a test outcome is positive means that you carry the virus, or did so in the past, and it is considered wise to go into quarantine for some time, to protect yourself and others. On the whole, the rise and fall of the positive rate is reflected in the rise and decline of both hospital admissions, IC admissions and deaths. Test outcomes therefore are considered to be a good, although somewhat indirect indicator of the spread of the virus throughout the population, even if it cannot distinguish clearly between those who are infectious and those who are not. 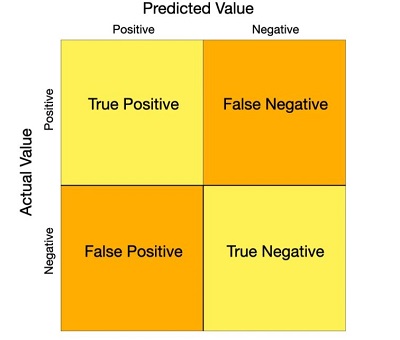
A confusion or error matrix of possible test outcomes.[2]
Mind you, this covers only the positive rate. What about the false positives? The number of false positives can never be higher than the number of positives. In general science estimates the number of PCR false positives to be very low, usually less than 1% and mostly caused by contamination or human error.[3] So it ranges from 0% (with a perfect test) to the percentage of positives measured (with a very lousy test)—and this last number can vary widely as we will see below. There is a lot of statistics involved here but that is not my point. This accepted view of science is attacked from many different angles—which are often mutually completely contradictory. So let's disentangle them here one by one. There is no virus...Given that our series of articles is about virus denialism, let's tackle that one first. If there is no virus, then strictly speaking 100% of all positive test outcomes must be false positives. But then, how is the fluctuation in test outcomes to be explained, if it no longer relates to the existence and spread of a real virus? Usually, it is claimed, without providing any empirical data, that these tests just detect human genetic material, present in our own cells. It is argued that this is most probably, because this particular virus hasn't been properly isolated before being sequenced, and instead cultured in cells that contain genetic material of their own. How can one possibly determine the origin of all this material? How can one be sure that the genetic material that is detected belongs to a virus? 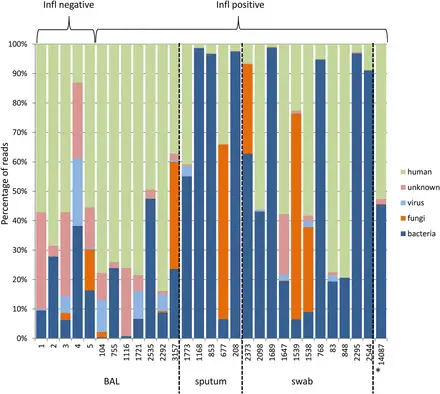
Next Generation Sequencing: human and non-human material.
The fact of the matter is that host RNA is filtered out when the sample taken from a patient or cell culture is sequenced. So science is of course aware that the sample contains a mix of many types of genetic material (from bacteria, fungi, viruses and humans), but that is not a problem at all. So any wild claim that "this may be all human genetic material we are testing for" sorely needs empirical support. Which isn't forthcoming. Too many cycles...Another argument frequently heard is that the PCR tests use so many so-called "cycles", that almost everybody will test positive. Kary Mullis, the inventor of the PCR test, is often quoted as saying "you can find almost anything in anyone", that is, if you test long enough. So the suggestion is, if you run 45 cycles (as recommended by the Drosten protocol), you will end up with close to 100% positive outcomes. It is also claimed that these very scientists warn against using too many cycles, and recommend not going beyond 35 cycles or so. So which is it? Are scientists aware that there is a major problem here and that they are unknowingly creating a "casedemic"? 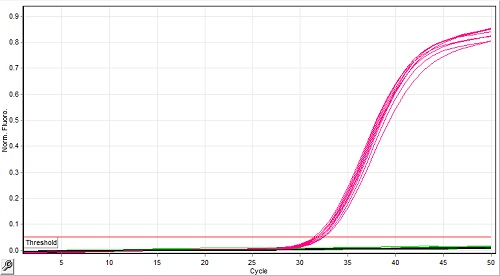
Most positive tests will turn positive long before the maximum number of cycles.[4]
This matter should be put to rest once and for all. It does not matter if you run a PCR test for 50 cycles or more.[4] The majority of positive tests will show their results much earlier. And the minority of cases that can only be found after running 35+ cycles are considered to be weak by scientists anyways. Since PCR runs in real time, the outcome can be read off during the cycling process. It shows a severe lack of understanding of PCR technology to claim that running 45 cycles turns into positive cases all the time. In the Corman-Drosten Review Report (see Part 20) we found this claim, which has been distributed widely in the conspiracy media: In case of virus detection, >35 cycles only detects signals which do not correlate with infectious virus as determined by isolation in cell culture; if someone is tested by PCR as positive when a threshold of 35 cycles or higher is used (as is the case in most laboratories in Europe & the US), the probability that said person is actually infected is less than 3%, the probability that said result is a false positive is 97% [4a] This leads to the following erroneous and hasty conclusions:
This study is often quoted in support of the mistaken conviction, that if the number of cycles exceeds 35, the percentage of infected persons is only 3%: 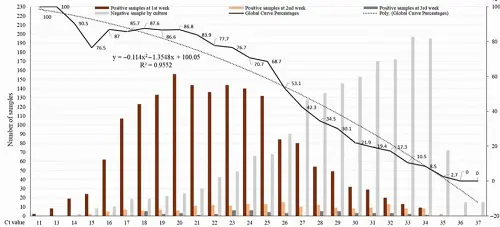
Percentage of positive viral cultures of severe acute respiratory syndrome coronavirus 2 polymerase chain reaction-positive nasopharyngeal samples from coronavirus disease 2019 patients, according to Ct value (plain line).[4a]
However, as you can see in the research graph, there was a wide range of observed Ct values, from 11 to 35 (with a peak at 20)! So it is not the case that if you run more than 35 cycles (which most test labs do), only 3% of the positive outcomes will be a True Positive. Rather, in those very rare cases where you really need so many cycles (>35) to see a signal at all, the chances of finding a viable virus is extremely low. See the difference? The gulf between science and pseudoscience could not be deeper. The PCR test sucks...Then again, it is sometimes argued that the PCR test is badly designed, so it produces artificial outcomes. It might for example have degenerate primers, which introduce some ambiguity in the way nucleotides are specified. Or the primer design is less than optimal, so the test even responds to its own primers. Or, that in the PCR products, when sequenced, the virus can be detected in only half of the cases.[4b] But then, if false positives are somehow produced by default, how can the percentage of positive tests fluctuate so widely (see below)? This makes no sense. Or, alternatively, the tests are not specific enough and respond to other viruses than only SARS-CoV-2, such as the common cold. Just check the first paper about PCR: 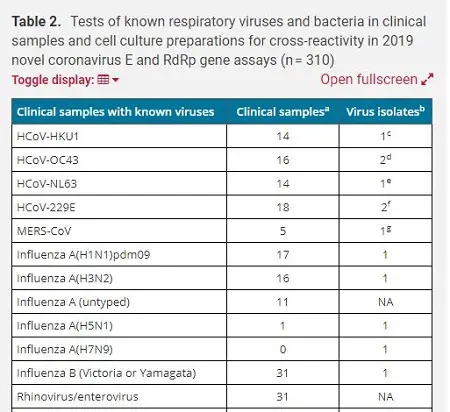
Partial view of the table of 22 known viruses the Drosten PCR test was tested for (including the common cold, MERS, influenza and rhinovirus).[5]
Again, this is an obsolete point that has been refuted multiple times. In this paper, testing for false positives was explicitly part of the protocol. Tests have been validated in many validation studies, and across the board are high in both specificity and sensitivity. The use of degenerate primers is standard practice, and is done to widen the scope of what can be detected (very prudent at the start of a pandemic when it is still unclear what viral enemy we are actually facing). Less-than-optimal primer design can cause problems but this will and should be corrected. The Drosten protocol deliberately aimed at viruses from the SARS family (though it also contained primers specific for SARS-CoV-2). It did not detect a slew of respiratory viruses, as documented in the original paper. Some smart ass critics claim that a PCR test can only detect viral fragments, and never the complete virus. That goes without saying. It is how PCR tests work. They look for signature sequences out of the total viral genome, like fingerprints. So this is not a bug, but a feature. Next. And finally, there are those who redefine "false positive" as meaning: you have the virus, but not enough to be infectious to others. Therefore, you don't need to be put in quarantine. Not so much a technical false positive but a clinical one. That too is a misreading of the data. For government policies to take effect, it is enough to have a suspicion of infectiousness, given the enormous impact if cases are missed. The positive truthAll these pseudoscientific arguments break down, because they would predict much higher percentages of positives around the world. And we don't see them. There are countries like New Zealand that consistently had 0.0% positives (and a corresponding low level of hospital admissions). After almost 14.000 tests! No positives—false or true does not really matter anymore. Here's a chart from June 2020, comparing different countries as to the percentage of tests that turned positive:[5] 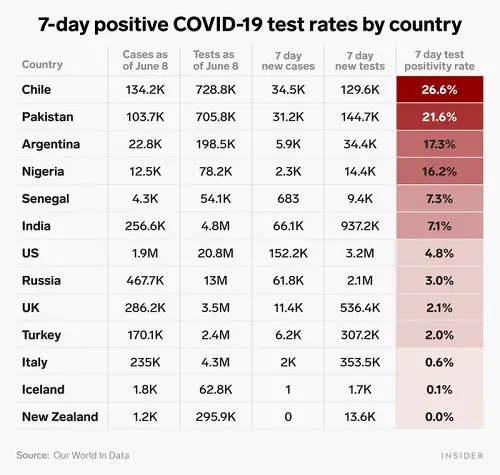
The positive percentages of PCR tests show a wide variety across countries.[6]
In those early days of the pandemic, the US was just below the recommended threshold of 5%, but many countries exceeded that, while other barely had any positives. How could these data possibly be explained within the virus denialist paradigm? It does not matter that these data are a year old to make this point. Did countries with close to zero positive percentages run less cycles? Nope. Did their inhabitants have different genetic material compared to other countries? Nope. Were countries with high positive percentages suffering from a flu pandemic? Nope. Did any of these countries run tests that were either superior or inferior to others? Nope. These patterns diverge not only between countries at a given moment in time, or between different regions of a country, but also across time within a given country, as you can see from this graph spanning the full pandemic: 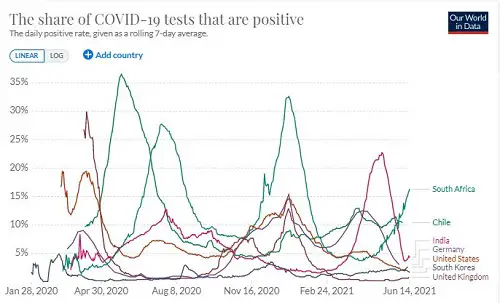
The positive rate: A crucial metric for understanding the pandemic.[7]
The huge variety of positive percentages in time and space matches more or less their health situation, hospital and IC admissions, as would be expected given the existence of a real virus and tests being reliable. Doubting the existence of the SARS-CoV-2 virus and/or the reliability of PCR tests has become thoroughly obselete. Coronavirus merchants of doubt will continue to sell their wares to the gullible, unfortunately, but their actions are unfounded and devoid of scientific credibility. Appendix 1: Wilson Debates LeeAt my request, Dan Wilson of Debunk the Funk debated with Sin Hang Lee, after Pieter Borger connected the two.
In this video recording, Wilson asks Lee repeatedly for evidence of his grand claims that the RT-qPCR tests currently in use produce a great many false positives. He shows him the data for Australia, where for months on a stretch almost no positive test outcomes were reported (let alone false positives). Lee repeatedly dodges this question, by saying he does not know, or that the false positives can be anywhere or everywhere, that the Australian data might be fabricated, or that in Australia the tests were withdrawn because of false positives—without providing any data. Lee also casts doubts on the specificity of the current tests. They might turn positive by matching any other virus, or some human genetic material. However, in the Corman-Drosten PCR protocol, may respiratory viruses were tested and none tested positive. Lee turns out to be a conspiracist, when he claims the relevant data are fabricated, science is corrupt and the PCR tests are useless. This is beyond any sense of rationality or evidence. Dan Wilson is to be recommended to keep his calm before a very agitated Sin Hang Lee. Highlight of the debate. After being confronted with data that contradict his prediction that there will always be many false positives, Lee continues to avoid the question: the data are manipulated, or computer generated, or hidden by corrupt governments. This is paranoia. Wilson nails it at the end of the 2-hour video, when emotions run high and Lee consistently avoids the data provided by Wilson. Lee: "I am trying to solve the pandemic." Wilson: "You are trying to solve a problem that does not exist." Lee concludes the conversation with a typical conspiracy argument: "You are trying to use government data to prove science, but that's not my approach." Wilson counters: it would be highly impractical to sequence every test results on a population scale, nor is it needed.
Wilson: "You are trying to solve a problem that does not exist."
Because so much time was spent/wasted on the unanswered false positives question, not all of these could be covered. NOTES[1] "Testing for COVID-19 - The positive rate: A crucial metric for understanding the pandemic", ourworldindata.org [2] Chia-Yi Hou, "False positive and false negative coronavirus test results explained", thehill.com [3] Andrew N. Cohen, "False Positives in PCR Tests for COVID-19", www.icd10monitor.com, November 9, 2020. [4] Ian M. MacKay, "The 'false-positive PCR' problem is not a problem", virologydownunder.com, Nov. 22, 2020, and "Putting PCR into real-time", virologydownunder.com, Jan. 2, 2021. [4a] Rita Jaafar et al., "Correlation Between 3790 Quantitative Polymerase Chain Reaction-Positives Samples and Positive Cell Cultures, Including 1941 Severe Acute Respiratory Syndrome Coronavirus 2 Isolates", Clinical Infectious Diseases, Volume 72, Issue 11, 1 June 2021. [4b] Pieter Borger was the first author of the "Corman-Drosten Review Report" (see Part 20). That report was titled "External peer review of the RTPCR test to detect SARS-CoV-2 reveals 10 major scientific flaws at the molecular and methodological level: consequences for false positive results" (emphasis added). His latest project is the promotion of molecular biologist Sin Hang Lee, who claims the qPCR tests produce 50% false positives by default due to hybridization or reacting to other viruses, human material, contamination, etc. These false positives are "built-in" so to speak, in Lee's opinion.  Lee has published two research articles, in open access/predatory journals:
Under Acknowledgement in this second paper we find this rather curious statement: "The manuscript of this article was initially submitted to the International Journal of Molecular Socieces Section "Molecular Diagnostics" and was rejected by Stephen A. Bustin, Section Editor in Chief, without peer reviews." Lee has a polemic with Bustin in this paper. Bustin, remember, was one of the reviewers of the Corman-Drosten retraction request paper submitted to Eurosurveillance (see Part 24) by the Borger-Kämmerer consortium. If such a large percentage of false positives is "built-in", as Sin Hang Lee claims, how can it be that some countries have had almost zero positive tests (not to mention false postive tests) for many months at a stretch? Key methodological question for Lee's research paper: is (Sanger) sequencing sensitive enough to detect the virus in diluted reference samples, especially since Lee tested samples with up to Ct=36.71? Above Ct=30 Sanger sequencing is less sensitive than qPCR. Could Lee's negative results be false negatives? (personal communication by @Rbor700 on Twitter) 
[5] Victor M Corman et. al., "Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR", PMC, www.ncbi.nlm.nih.gov, (Euro Surveillance, 2020 Jan 23). [6] Tyler Sonnemaker,"One chart shows what percentage of COVID-19 tests are coming back positive in the US compared to 12 other countries", businessinsider.com, Jun 12, 2020. [7] "The positive rate: A crucial metric for understanding the pandemic", ourworldindata.org [8] Sin Hang Lee, "PCR is a tool for DNA replication: Debunk the Funk with Dr. Wilson on SARS-CoV-2 PCR diagnostics", Powerpoint, 64 pages, December 4, 2021.
83 Vaccine Myths from docbastard.net
To all those who claim SARS-CoV-2—or any virus—does not exist: the virosphere consists of 7 realms
11 kingdoms, 22 phyla, 4 subphyla, 49 classes, 93 orders, 12 suborders, 368 families, 213 subfamilies, 3,769 genera, 86 subgenera, 16,215 species. Take that.
https://talk.ictvonline.org/taxonomy/
A summary of early parts of this series has appeared in the Dutch magazine Skepter 33(3), September 2020, as "Viruses don't exist" (covering Parts 1-5). German: Skeptiker (December 2020); English: Skeptic.org.uk (January 2021)
Comment Form is loading comments...
|